
Musculoskeletal Imaging / Cartilage Repair
Cartilage Repair
Imaging in Cartilage Repair
As cartilage injuries are common and frequently affect young patients with potential for progression to osteoarthritis, treatment to alleviate symptoms and potentially delay joint degeneration is warranted. A number of surgical techniques are available to treat focal chondral defects including marrow stimulation, osteochondral auto- and allografting, and autologous chondrocyte implantation. Although arthroscopy is considered the gold standard for evaluation of cartilage pre- and post repair, it is invasive with associated morbidity and cannot adequately assess the deep cartilage layer and underlying bone.
Magnetic resonance imaging provides unparalleled non-invasive assessment of the repair site and all other joint tissues. Several techniques and methods are available to evaluate the success of cartilage repair strategies in a clinical trial setting that are offered by BICL and are performed by our leading imaging experts.




MRI Observation of Cartilage Repair Tissue (MOCART).
MOCART provides a reproducible semi-quantitative scoring system for morphological cartilage repair assessment that has been widely used as an outcome measure for longitudinal clinical trials. MOCART originally defined 9 structural variables but was modified and expanded to assess 11 variables to take advantage of higher resolution 2D images and isotropic 3D MR sequences. The -MOCART improves evaluation of repair tissue by localizing the features within the repair site and evaluating the border zones of the repair tissue-cartilage interfaces in every plane, and the relation of the repair site to the weight-bearing regions of the joint. A detailed assessment of the subchondral bone was also incorporated. Since all features of the original MOCART are assessed also by 3D-MOCART, we only describe the 3D-MOCART features.
Cartilage Repair Osteoarthritis Knee Score (CROAKS).
Although the 3D MOCART is excellent for assessment of the repair site, it largely ignores the rest of the joint, which may be of relevance especially n longitudinal follow-up. MRI osteoarthritis knee score (MOAKS) is an established semi-quantitative scoring system for whole organ assessment of the joint that is not able to integrate detailed information on the repair site and immediate surroundings. As a consequence BICL members have developed the cartilage repair OA knee score (CROAKS) instrument to combine features of these two scores to provide an a comprehensive, reproducible tool for longitudinal postoperative whole-organ assessment after surgical cartilage repair using a multi-subregion division of the joint.
In addition to the previously described repair tissue features evaluated by 3D MOCART, the whole-organ characteristics assessed by CROAKS include; bone marrow lesions (BMLS) beyond the repair site, subchondral cysts, cartilage status beyond the repair site, osteophytes, synovitis, effusion, menisci, and anterior and posterior cruciate ligaments (ACL and PCL). Some of the other periarticular features evaluated include the pes anserine bursa, illiotibial band, prepatellar bursa, infrapatellar bursa, and presence of popliteal cysts, ganglion cysts or loose bodies.
Cartilage Repair Osteoarthritis Knee Score (CROAKS), developed by BICL’s leading imaging experts, optimizes whole organ assessment of the joint after cartilage repair by combining features of these two scores. An overview of the different dimensions of the CROAKS score is presented below.
Illustrative Cases using CROAKS grading scheme
-
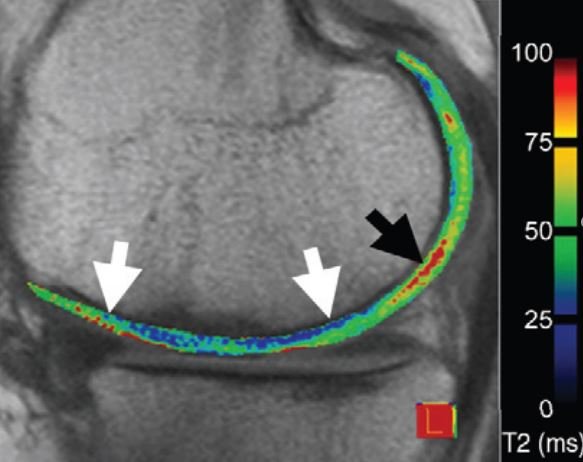
Multi-tissue assessment
Coronal dual echo at steady state (DESS) image shows 24 months follow up examination after MACI of the medial weight bearing femur (large arrows). Partial underfilling of the repair zone is noted. In addition large marginal osteophytes characteristic of definite osteoarthritis are noted at the medial and lateral tibio-femorla joint (small arrows). These osseous bone outgrowths are not assessed in grading schemes focusing on the repair zone only.
-

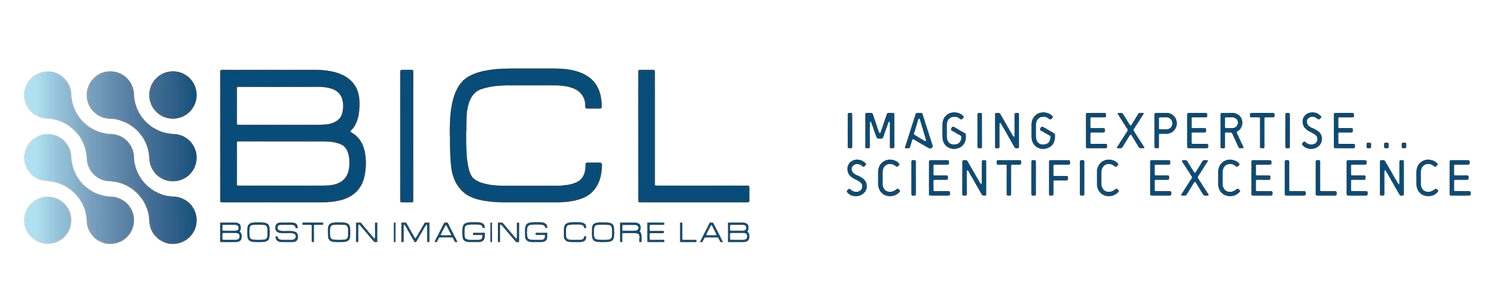
Cartilage assessment
Sagittal proton density weighted image shows the lateral tibio-femoral compartment 18 months after MACI of the lateral weight bearing femur. The repair zone is demarcated by long thin arrows and hypertrophy of the repair tissue is noted. At the posterior lateral tibia, there is a focal areaq of superficial cartilage thjinning and marked intrachondral hyperintensity of the native cartilage (large arrow). This finding of pathology distant to the repair zone is not covered by commonly applied cartilage repair grading schemes but might be relevant for long term outcome of the joint.
Individual Features of the CROAKS system
Variable:
-
Grading
Bone marrow edema lesions and subchondral cysts are assessed together as they share common pathophysiology. These are both graded in 15 standardized subregions of the knee.
Percentage of the volume of each BML that is BML (as distinct from cyst) is graded as; Grade 0= none
Grade 1 <25%
Grade 2= 25-50%
Grade 3 >50%
If a cyst is present without an associated bone marrow lesion then cysts will be scored as a 0 for size % of lesion that is BML.
-
The cartilage is graded in 14 described subregions for areal extent of cartilage loss and % of loss within this subregion, which is full thickness.
A two digit score is given to each subregion with the first digit describing size of lesion and the second digit describing percentage of subregion that is affected by full thickness loss.
-
Osteophytes are scored in 12 locations according to size from grades 0 to 3; along the trochlea, central weight bearing and posterior margins of the femoral condyles and weight bearing tibial plateaus, and along the medial, lateral, superior and inferior margins of the patella. Posterior femoral osteophytes are assessed peripherally and centrally. The larger osteophyte for either, peripheral or central location is scored.
-
As contrast-enhanced sequences are not currently employed in large studies assessing cartilage repair, a surrogate of signal changes in Hoffa’s fat pad has been applied that has been shown on biopsy to represent mild chronic synovitis (159). This abnormality is best described as diffuse hyperintense signal on T2, PD, and IW fat suppressed sequences within the fat pad. In addition to synovitis these signal changes could also be attributed to other etiologies such as post-arthroscopic changes or Hoffa’s disease (160).
Hoffa-synovitis score is scored on a mid-line sagittal image as one single score for assessment of degree of hyperintensity in Hoffa’s fat pad based on the region outlined in Scoring is based on size:
Grade 0= normal
Grade 1= mild
Grade 2= moderate
Grade 3= severe
Knees that have undergone a cartilage repair procedure often show scarring in Hoffa’s fat pad with concurrent signal alterations on MRI. These signal changes cannot be distinguished from true synovitis, as only contrast-enhanced MRI is able to differentiate between active inflammation and inactive scar tissue.
-
Changes in meniscal position and meniscal morphologic changes manifesting as tears or loss of substance have both been shown to predispose to cartilage loss (161, 162).
Meniscal extrusion is graded in four locations as follows:
Medial Meniscus: Medial extrusion relative to medial tibial margin (coronal image)
Medial Meniscus: Anterior extrusion (sagittal image) where extrusion is maximum
Lateral Meniscus: Lateral extrusion relative to lateral tibial margin (coronal image)
Lateral Meniscus: Anterior extrusion (sagittal image) where extrusion is maximum
The reference for measurement is the edge of the tibial plateau (excluding osteophyte). Extrusion is scored as follows:
Grade 0 - no extrusion
Grade 1 - < 2mm
Grade 2 - 2-5 mm
Grade 3 - > 5mm
Morphology is assessed for the medial and lateral meniscus at the anterior, body and posterior horn. The anterior and posterior horn regions are scored using the sagittal sequences and the body is scored using the coronal sequences. Morphologic features are scored as follows:
Grade 0: Normal
Grade 1 - High signal not extending through meniscal surface i.e. not a tear
Grade 2 - Horizontal tear: grade 0 - absent, grade 1 – present
Grade 3 - Radial Tear: grade 0 - absent, grade 1 – present
Grade 4 - Longitudinal tear: grade 0 - absent, grade 1 – present
Grade 5 - Complex tear: grade 0 - absent, grade 1 - present
Defined by high signal that extends to 2 surfaces and > 3 points
Grade 6 - Root tear (posterior horn): grade 0 - absent, grade 1 - present
Grade 7 - Partial maceration: grade 0 - absent, grade 1 - present
Defined by loss of morphological substance of the meniscus
Grade 8 - Progressive partial maceration: grade 0 - absent, grade 1 – present
Progressive partial maceration as compared to the previous visit.
Grade 9 - Complete maceration: No more meniscal substance visible.
Meniscal cyst: grade 0 - absent, grade 1 - present
Meniscal hypertrophy: grade 0 - absent, grade 1 – present
Defined as definite increase in meniscal volume in given subregion when compared to normal
-
The ligaments are graded as follows:
a) Anterior Cruciate Ligament (ACL)
Grade 0: normal
Grade 1: partial tear
Grade 2: complete tear
b) Associated with BML/cyst at site of ACL insertion or origin
Grade 0: absent
Grade 1: present
c) ACL Repair
Grade 0: absent
Grade 1: present
d) Posterior Cruciate Ligament (PCL)
Grade 0: normal
Grade 1: complete tear
e) Associated with BML/cyst at site of PCL insertion or origin
Grade 0: absent
Grade 1: present
f) Patellar tendon
Grade 0: no signal abnormality
Grade 2: signal abnormality present
-
Some of the other periarticular features assessed are as follows:
a) Pes anserine bursitis
Grade 0- absent
Grade 1-present
b) Illiotibial band signal (bursitis)
Grade 0- absent
Grade 1- present
Popliteal cyst
Grade 0- absent
Grade 1- present
c) Infrapatellar bursa signal (bursitis)
Grade 0-absent
Grade 1-present
d) Prepatellar bursa signal (bursitis)
Grade 0 - absent
Grade 1 – present
e) Ganglion cyst
Associated with the tibio-fibular joint: grade 0 - absent, grade 1 - present
Associated with PCL and ACL: grade 0 - absent, grade 1 - present
Other: grade 0 - absent, grade 1 – present
f) Loose bodies
Grade 0 - absent
Grade 1 - present